Can Two a Positiveblood Types Have a a Negative Baby

Blood type (or blood group) is determined, in function, past the ABO blood grouping antigens present on red blood cells.
A blood blazon (also known every bit a blood group) is a classification of blood, based on the presence and absence of antibodies and inherited antigenic substances on the surface of red blood cells (RBCs). These antigens may be proteins, carbohydrates, glycoproteins, or glycolipids, depending on the blood group system. Some of these antigens are too present on the surface of other types of cells of diverse tissues. Several of these carmine blood cell surface antigens tin stalk from one allele (or an alternative version of a gene) and collectively class a blood group system.[one]
Blood types are inherited and represent contributions from both parents of an individual. As of 2021[update], a total of 43 man blood grouping systems are recognized by the International Gild of Claret Transfusion (ISBT).[2] The two most of import blood group systems are ABO and Rh; they determine someone'southward blood type (A, B, AB, and O, with + or - cogent RhD status) for suitability in blood transfusion.
Blood group systems [edit]
A complete blood type would describe each of the 43 blood groups, and an private'southward claret type is 1 of many possible combinations of blood-group antigens.[2] Almost always, an private has the same blood grouping for life, but very rarely an individual's blood type changes through addition or suppression of an antigen in infection, malignancy, or autoimmune disease.[3] [4] [5] [6] Another more than mutual cause of blood type change is a os marrow transplant. Bone-marrow transplants are performed for many leukemias and lymphomas, among other diseases. If a person receives bone marrow from someone of a different ABO blazon (e.chiliad., a type A patient receives a type O bone marrow), the patient's blood type should eventually becomes the donor's type, as the patient'southward hematopoietic stem cells (HSCs) are destroyed, either by ablation of the bone marrow or past the donor's T-cells. Once all the patient'due south original cerise blood cells accept died, they volition have been fully replaced by new cells derived from the donor HSCs. Provided the donor had a different ABO type, the new cells' surface antigens will be different from those on the surface of the patient's original reddish blood cells.[ citation needed ]
Some blood types are associated with inheritance of other diseases; for example, the Kell antigen is sometimes associated with McLeod syndrome.[7] Certain claret types may touch susceptibility to infections, an example being the resistance to specific malaria species seen in individuals defective the Duffy antigen.[8] The Duffy antigen, presumably as a result of natural option, is less common in population groups from areas having a high incidence of malaria.[ix]
ABO claret group system [edit]

ABO blood group organization: diagram showing the carbohydrate chains that determine the ABO claret group
The ABO claret group organisation involves ii antigens and two antibodies found in human blood. The two antigens are antigen A and antigen B. The two antibodies are antibody A and antibody B. The antigens are nowadays on the cherry-red blood cells and the antibodies in the serum. Regarding the antigen property of the blood all human beings can be classified into 4 groups, those with antigen A (grouping A), those with antigen B (group B), those with both antigen A and B (group AB) and those with neither antigen (grouping O). The antibodies present together with the antigens are found as follows:[ citation needed ]
- Antigen A with antibody B
- Antigen B with antibody A
- Antigen AB has no antibodies
- Antigen zip (group O) with antibody A and B.
In that location is an agglutination reaction betwixt similar antigen and antibiotic (for instance, antigen A agglutinates the antibiotic A and antigen B agglutinates the antibody B). Thus, transfusion can be considered rubber as long every bit the serum of the recipient does non incorporate antibodies for the blood cell antigens of the donor.[ citation needed ]
The ABO arrangement is the most important claret-grouping organization in human-blood transfusion. The associated anti-A and anti-B antibodies are usually immunoglobulin M, abbreviated IgM, antibodies. It has been hypothesized that ABO IgM antibodies are produced in the offset years of life by sensitization to ecology substances such equally food, leaner, and viruses, although claret group compatibility rules are practical to newborn and infants as a matter of do.[ten] The original terminology used by Karl Landsteiner in 1901 for the nomenclature was A/B/C; in later publications "C" became "O".[xi] Type O is often called 0 (cypher, or nil) in other languages.[11] [12]
Rh blood group system [edit]
The Rh system (Rh meaning Rhesus) is the second most pregnant claret-grouping organisation in man-claret transfusion with currently 50 antigens. The near significant Rh antigen is the D antigen, because it is the most likely to provoke an immune system response of the five main Rh antigens. It is common for D-negative individuals not to have any anti-D IgG or IgM antibodies, because anti-D antibodies are non usually produced by sensitization against ecology substances. Nevertheless, D-negative individuals can produce IgG anti-D antibodies following a sensitizing effect: peradventure a fetomaternal transfusion of claret from a fetus in pregnancy or occasionally a claret transfusion with D positive RBCs.[xiii] Rh disease tin can develop in these cases.[14] Rh negative claret types are much less mutual in Asian populations (0.three%) than they are in European populations (15%).[15] The presence or absence of the Rh(D) antigen is signified by the + or − sign, and so that, for example, the A− group is ABO type A and does not accept the Rh (D) antigen.[ citation needed ]
ABO and Rh distribution by country [edit]
As with many other genetic traits, the distribution of ABO and Rh blood groups varies significantly betwixt populations.[ citation needed ]
Other blood group systems [edit]
As of 2021[update], 41 blood-group systems have been identified by the International Society for Blood Transfusion in addition to the ABO and Rh systems.[2] Thus, in addition to the ABO antigens and Rh antigens, many other antigens are expressed on the RBC surface membrane. For case, an individual tin can exist AB, D positive, and at the same time Thousand and N positive (MNS organization), K positive (Kell system), Lea or Leb negative (Lewis system), and so on, existence positive or negative for each blood group arrangement antigen. Many of the blood grouping systems were named after the patients in whom the corresponding antibodies were initially encountered. Claret group systems other than ABO and Rh pose a potential, yet relatively low, take chances of complications upon mixing of blood from unlike people.[16]
Following is a comparing of clinically relevant characteristics of antibodies against the main human being blood group systems:[17]
| ABO | Rh | Kell | Duffy | Kidd | |
|---|---|---|---|---|---|
| Naturally occurring | Yeah | No | No | No | No |
| Most common in immediate hemolytic transfusion reactions | A | Yep | Fya | Jka | |
| Most mutual in delayed hemolytic transfusion reactions | E,D,C | Jka | |||
| Most mutual in hemolytic illness of the newborn | Yep | D,C | Aye | ||
| Commonly produce intravascular hemolysis | Yes | Yes |
Clinical significance [edit]
Blood transfusion [edit]
Transfusion medicine is a specialized branch of hematology that is concerned with the study of blood groups, along with the work of a blood bank to provide a transfusion service for blood and other claret products. Beyond the world, claret products must be prescribed by a medical doc (licensed physician or surgeon) in a like fashion as medicines.[ citation needed ]

Much of the routine work of a claret bank involves testing blood from both donors and recipients to ensure that every individual recipient is given blood that is compatible and is as safety as possible. If a unit of incompatible blood is transfused between a donor and recipient, a severe acute hemolytic reaction with hemolysis (RBC devastation), kidney failure and shock is probable to occur, and death is a possibility. Antibodies can be highly active and can set on RBCs and bind components of the complement system to cause massive hemolysis of the transfused claret.[ citation needed ]
Patients should ideally receive their own claret or type-specific blood products to minimize the hazard of a transfusion reaction. It is as well possible to use the patient'south own claret for transfusion. This is called autologous blood transfusion, which is always compatible with the patient. The procedure of washing a patient'southward ain carmine blood cells goes as follows: The patient's lost claret is nerveless and washed with a saline solution. The washing procedure yields concentrated washed red blood cells. The last step is reinfusing the packed red claret cells into the patient. There are multiple ways to wash cherry-red blood cells. The two main ways are centrifugation and filtration methods. This procedure can be performed with microfiltration devices like the Hemoclear filter. Risks can be further reduced past cross-matching blood, but this may exist skipped when claret is required for an emergency. Cross-matching involves mixing a sample of the recipient's serum with a sample of the donor's ruby-red claret cells and checking if the mixture agglutinates, or forms clumps. If agglutination is non obvious by directly vision, blood bank technicians unremarkably check for agglutination with a microscope. If agglutination occurs, that item donor's blood cannot be transfused to that item recipient. In a blood banking company it is vital that all blood specimens are correctly identified, so labelling has been standardized using a barcode system known as ISBT 128.
The blood grouping may be included on identification tags or on tattoos worn past military personnel, in case they should need an emergency blood transfusion. Frontline German Waffen-SS had claret group tattoos during World War II.
Rare blood types tin crusade supply problems for blood banks and hospitals. For example, Duffy-negative blood occurs much more frequently in people of African origin,[xx] and the rarity of this claret blazon in the residual of the population can result in a shortage of Duffy-negative blood for these patients. Similarly, for RhD negative people there is a risk associated with travelling to parts of the world where supplies of RhD negative blood are rare, particularly East Asia, where blood services may endeavor to encourage Westerners to donate claret.[21]
Hemolytic disease of the newborn (HDN) [edit]
A pregnant woman may carry a fetus with a blood type which is different from her own. Typically, this is an issue if a Rh- female parent has a child with a Rh+ father, and the fetus ends up being Rh+ like the male parent.[22] In those cases, the mother can make IgG blood grouping antibodies. This tin happen if some of the fetus' blood cells pass into the mother's blood circulation (e.g. a small fetomaternal hemorrhage at the time of childbirth or obstetric intervention), or sometimes later a therapeutic blood transfusion. This tin can cause Rh disease or other forms of hemolytic disease of the newborn (HDN) in the electric current pregnancy and/or subsequent pregnancies. Sometimes this is lethal for the fetus; in these cases information technology is chosen hydrops fetalis.[23] If a pregnant adult female is known to have anti-D antibodies, the Rh claret type of a fetus tin can be tested by assay of fetal DNA in maternal plasma to assess the chance to the fetus of Rh disease.[24] One of the major advances of twentieth century medicine was to foreclose this disease by stopping the germination of Anti-D antibodies by D negative mothers with an injectable medication chosen Rho(D) immune globulin.[25] [26] Antibodies associated with some claret groups can cause severe HDN, others can only cause mild HDN and others are not known to cause HDN.[23]
Blood products [edit]
To provide maximum benefit from each blood donation and to extend shelf-life, blood banks fractionate some whole claret into several products. The almost mutual of these products are packed RBCs, plasma, platelets, cryoprecipitate, and fresh frozen plasma (FFP). FFP is quick-frozen to retain the labile clotting factors V and VIII, which are ordinarily administered to patients who take a potentially fatal clotting problem caused past a condition such as advanced liver affliction, overdose of anticoagulant, or disseminated intravascular coagulation (DIC).[ citation needed ]
Units of packed ruby-red cells are made by removing every bit much of the plasma every bit possible from whole blood units.
Clotting factors synthesized by modern recombinant methods are now in routine clinical use for hemophilia, as the risks of infection transmission that occur with pooled blood products are avoided.
Red blood cell compatibility [edit]
- Blood group AB individuals have both A and B antigens on the surface of their RBCs, and their blood plasma does not incorporate whatsoever antibodies confronting either A or B antigen. Therefore, an private with type AB claret tin receive blood from any group (with AB being preferable), but cannot donate blood to any group other than AB. They are known as universal recipients.
- Blood grouping A individuals have the A antigen on the surface of their RBCs, and blood serum containing IgM antibodies against the B antigen. Therefore, a group A private tin can receive blood only from individuals of groups A or O (with A being preferable), and can donate claret to individuals with type A or AB.
- Claret group B individuals have the B antigen on the surface of their RBCs, and blood serum containing IgM antibodies against the A antigen. Therefore, a group B individual can receive blood just from individuals of groups B or O (with B being preferable), and can donate blood to individuals with type B or AB.
- Blood grouping O (or blood grouping cipher in some countries) individuals exercise non have either A or B antigens on the surface of their RBCs, and their blood serum contains IgM anti-A and anti-B antibodies. Therefore, a group O individual tin can receive blood only from a group O private, just can donate blood to individuals of whatsoever ABO claret group (i.e., A, B, O or AB). If a patient needs an urgent blood transfusion, and if the fourth dimension taken to process the recipient's blood would cause a detrimental delay, O negative claret can be issued. Considering it is compatible with anyone, O negative blood is often overused and consequently is ever in brusque supply.[27] According to the American Association of Blood Banks and the British Chief Medical Officeholder's National Claret Transfusion Committee, the utilize of group O RhD negative cerise cells should be restricted to persons with O negative blood, women who might be pregnant, and emergency cases in which claret-group testing is genuinely impracticable.[27]
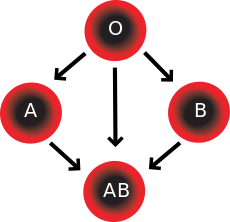
Red claret jail cell compatibility nautical chart
In improver to altruistic to the same blood grouping; blazon O blood donors can give to A, B and AB; claret donors of types A and B tin give to AB.
| Recipient[ane] | Donor[1] | |||||||
|---|---|---|---|---|---|---|---|---|
| O− | O+ | A− | A+ | B− | B+ | AB− | AB+ | |
| O− | | | | | | | | |
| O+ | | | | | | | | |
| A− | | | | | | | | |
| A+ | | | | | | | | |
| B− | | | | | | | | |
| B+ | | | | | | | | |
| AB− | | | | | | | | |
| AB+ | | | | | | | | |
Table note
1. Assumes absence of atypical antibodies that would cause an incompatibility between donor and recipient blood, as is usual for claret selected by cross matching.
An Rh D-negative patient who does non have whatsoever anti-D antibodies (never existence previously sensitized to D-positive RBCs) tin can receive a transfusion of D-positive blood one time, but this would cause sensitization to the D antigen, and a female patient would get at take chances for hemolytic disease of the newborn. If a D-negative patient has developed anti-D antibodies, a subsequent exposure to D-positive claret would lead to a potentially dangerous transfusion reaction. Rh D-positive blood should never exist given to D-negative women of changeable age or to patients with D antibodies, so blood banks must conserve Rh-negative blood for these patients. In extreme circumstances, such equally for a major drain when stocks of D-negative blood units are very low at the claret bank, D-positive blood might be given to D-negative females higher up child-bearing historic period or to Rh-negative males, providing that they did non take anti-D antibodies, to conserve D-negative blood stock in the blood bank. The antipodal is not true; Rh D-positive patients do not react to D negative blood.
This same matching is washed for other antigens of the Rh system as C, c, E and e and for other blood group systems with a known risk for immunization such as the Kell system in particular for females of child-bearing age or patients with known demand for many transfusions.
Plasma compatibility [edit]
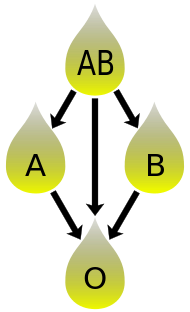
Plasma compatibility nautical chart
In add-on to altruistic to the aforementioned blood group; plasma from blazon AB tin be given to A, B and O; plasma from types A, B and AB can be given to O.
Blood plasma compatibility is the changed of scarlet claret cell compatibility.[30] Blazon AB plasma carries neither anti-A nor anti-B antibodies and can be transfused to individuals of any blood grouping; merely type AB patients can merely receive type AB plasma. Type O carries both antibodies, so individuals of blood group O can receive plasma from whatsoever blood group, just type O plasma tin be used just by blazon O recipients.
| Recipient | Donor | |||
|---|---|---|---|---|
| O | A | B | AB | |
| O | | | | |
| A | | | | |
| B | | | | |
| AB | | | | |
Table annotation
ane. Assuming absenteeism of strong atypical antibodies in donor plasma
Rh D antibodies are uncommon, so generally neither D negative nor D positive blood contain anti-D antibodies. If a potential donor is institute to have anti-D antibodies or any strong atypical blood group antibody by antibody screening in the blood banking company, they would not be accepted every bit a donor (or in some blood banks the blood would be drawn but the product would need to be appropriately labeled); therefore, donor claret plasma issued past a blood banking company tin can be selected to exist gratis of D antibodies and costless of other atypical antibodies, and such donor plasma issued from a blood bank would exist suitable for a recipient who may be D positive or D negative, as long as blood plasma and the recipient are ABO uniform.[ citation needed ]
Universal donors and universal recipients [edit]

A infirmary worker takes samples of blood from a donor for testing
In transfusions of packed red blood cells, individuals with blazon O Rh D negative claret are often called universal donors. Those with type AB Rh D positive blood are chosen universal recipients. However, these terms are just generally truthful with respect to possible reactions of the recipient's anti-A and anti-B antibodies to transfused ruddy claret cells, and likewise possible sensitization to Rh D antigens. Ane exception is individuals with hh antigen organisation (also known as the Mumbai phenotype) who tin can merely receive blood safely from other hh donors, because they class antibodies against the H antigen present on all cherry blood cells.[32] [33]
Blood donors with exceptionally strong anti-A, anti-B or any atypical claret grouping antibiotic may be excluded from blood donation. In full general, while the plasma fraction of a blood transfusion may carry donor antibodies non constitute in the recipient, a pregnant reaction is unlikely because of dilution.
Additionally, cherry claret jail cell surface antigens other than A, B and Rh D, might cause agin reactions and sensitization, if they tin can demark to the respective antibodies to generate an immune response. Transfusions are further complicated because platelets and white blood cells (WBCs) have their own systems of surface antigens, and sensitization to platelet or WBC antigens tin occur every bit a effect of transfusion.
For transfusions of plasma, this state of affairs is reversed. Type O plasma, containing both anti-A and anti-B antibodies, can only be given to O recipients. The antibodies will assault the antigens on any other blood type. Conversely, AB plasma tin be given to patients of whatsoever ABO blood grouping, considering it does not incorporate any anti-A or anti-B antibodies.
Claret typing [edit]
Typically, claret type tests are performed through addition of a blood sample to a solution containing antibodies corresponding to each antigen. The presence of an antigen on the surface of the blood cells is indicated by agglutination. In these tests, rather than agglutination, a positive result is indicated by decolorization equally red blood cells which bind to the nanoparticles are pulled toward a magnet and removed from solution.
Blood grouping genotyping [edit]
In addition to the current do of serologic testing of blood types, the progress in molecular diagnostics allows the increasing use of blood group genotyping. In contrast to serologic tests reporting a direct blood type phenotype, genotyping allows the prediction of a phenotype based on the knowledge of the molecular ground of the currently known antigens. This allows a more detailed determination of the blood type and therefore a improve match for transfusion, which can be crucial in particular for patients with needs for many transfusions to forbid allo-immunization.[34] [35]
History [edit]
Blood types were first discovered by an Austrian physician, Karl Landsteiner, working at the Pathological-Anatomical Establish of the University of Vienna (at present Medical Academy of Vienna). In 1900, he found that blood sera from unlike persons would clump together (agglutinate) when mixed in test tubes, and not merely that, some human claret also agglutinated with animate being blood.[36] He wrote a two-sentence footnote:
The serum of good for you man beings not only agglutinates animal red cells, but also often those of human origin, from other individuals. Information technology remains to exist seen whether this advent is related to inborn differences between individuals or it is the result of some damage of bacterial kind.[37]
This was the first show that blood variation exists in humans. The next yr, in 1901, he made a definitive ascertainment that claret serum of an private would agglutinate with only those of sure individuals. Based on this he classified human bloods into three groups, namely group A, group B, and group C. He defined that grouping A blood agglutinates with group B, but never with its own blazon. Similarly, group B blood agglutinates with grouping A. Grouping C claret is different in that it agglutinates with both A and B.[38] This was the discovery of claret groups for which Landsteiner was awarded the Nobel Prize in Physiology or Medicine in 1930. (C was afterward renamed to O after the German Ohne, meaning without, or zero, or null.[39]) Another group (later on named AB) was discovered a year later past Landsteiner'due south students Adriano Sturli and Alfred von Decastello without designating the proper name (simply referring it to as "no particular type").[40] [41] Thus, later on Landsteiner, three blood types were initially recognised, namely A, B, and C.[41]
Czech serologist January Janský was the first to recognise and designate iv blood types in 1907 that he published in a local journal,[42] using the Roman numerical I, II, Three, and IV (respective to modern O, A, B, and AB respectively).[43] Unknown to Janský, an American physician William L. Moss introduced well-nigh identical nomenclature in 1910;[44] merely his I and IV corresponding Janský's 4 and I.[45] Moss came across Janský's paper as his was being printed, mentioned it in a footnote.[41] Thus the existence of two systems immediately created confusion and potential danger in medical do. Moss'due south system was adopted in Britain, France, and U.s.a., while Janský's was preferred in most other European countries and some parts of US. It was reported that "The practically universal use of the Moss classification at that time was completely and purposely cast aside. Therefore in place of bringing order out of chaos, anarchy was increased in the larger cities."[46] To resolve the confusion, the American Association of Immunologists, the Society of American Bacteriologists, and the Association of Pathologists and Bacteriologists made a joint recommendation in 1921 that the Jansky classification be adopted based on priority.[47] Just it was not followed particularly where Moss'due south system had been used.[48]
In 1927, Landsteiner, who had moved to the Rockefeller Institute for Medical Research in New York, and as a member of a committee of the National Enquiry Council concerned with claret grouping suggested to substitute Janský's and Moss's systems with the letters O, A, B, and AB. In that location was some other confusion on the use of O which was introduced past Polish physicians Ludwik Hirszfeld and German physician Emil von Dungern in 1910.[49] It was never clear whether it was meant for the effigy 0, German nix for zero or the upper instance letter O for ohne, meaning without; Landsteiner chose the latter.[50]
In 1928 the Permanent Commission on Biological Standardization adopted Landsteiner's proposal and stated:
The Committee learns with satisfaction that, on the initiative of the Health Organization of the League of Nations, the classification proposed by von Dungern and Hirszfeld for the classification of blood groups has been by and large accepted, and recommends that this nomenclature shall be adopted for international utilise as follows: 0 A B AB. To facilitate the change from the nomenclature hitherto employed the following is suggested:
- Jansky ....0(I) A(Ii) B(Three) AB(IV)
- Moss ... O(IV) A(Two) B(3) AB(I)[51]
This nomenclature became widely accepted; however, non all hospitals and doctors used blood typing for transfusion even in the late 1940s. The new arrangement was gradually accustomed and by the early 1950s, it was universally followed.[52]
Hirszfeld and Dungern discovered the inheritance of blood types equally Mendelian genetics in 1910 and the existence of sub-types of A in 1911.[49] [53] In 1927, Landsteiner, with Philip Levine, discovered the MN claret grouping system,[54] and the P system.[55] Development of the Coombs test in 1945,[56] the advent of transfusion medicine, and the understanding of ABO hemolytic affliction of the newborn led to discovery of more blood groups. Every bit of 2020[update], the International Order of Blood Transfusion (ISBT) recognizes 41 blood groups.[2]
Gild and culture [edit]
A popular pseudoscientific belief in Eastern Asian countries (particularly in Japan and Korea;[57] known as 血液型 ketsuekigata / hyeoraekhyeong) is that a person's ABO claret type is predictive of their personality, character, and compatibility with others.[58] Researchers have established no scientific ground exists for claret type personality categorization, and studies have found no "significant human relationship betwixt personality and blood type, rendering the theory "obsolete" and concluding that no basis exists to assume that personality is anything more than randomly associated with blood type."[57]
Come across as well [edit]
- Claret blazon (non-human)
- Human leukocyte antigen
- hh blood grouping
References [edit]
- ^ Maton, Anthea; Jean Hopkins; Charles William McLaughlin; Susan Johnson; Maryanna Quon Warner; David LaHart; Jill D. Wright (1993). Human Biology and Health . Englewood Cliffs NJ: Prentice Hall. ISBN0-13-981176-one.
- ^ a b c d "Red Jail cell Immunogenetics and Blood Group Terminology". International Society of Blood Transfusion. 2021. Archived from the original on 11 February 2022. Retrieved 11 February 2022.
- ^ Dean 2005, The ABO claret group "... A number of illnesses may alter a person's ABO phenotype ..."
- ^ Stayboldt C, Rearden A, Lane TA (1987). "B antigen caused by normal A1 blood-red cells exposed to a patient'southward serum". Transfusion. 27 (one): 41–iv. doi:10.1046/j.1537-2995.1987.27187121471.x. PMID 3810822. S2CID 38436810.
- ^ Matsushita Southward, Imamura T, Mizuta T, Hanada M (November 1983). "Caused B antigen and polyagglutination in a patient with gastric cancer". The Japanese Journal of Surgery. 13 (6): 540–2. doi:ten.1007/BF02469500. PMID 6672386. S2CID 6018274.
- ^ Kremer Hovinga I, Koopmans M, de Heer E, Bruijn J, Bajema I (2007). "Change in blood group in systemic lupus erythematosus". Lancet. 369 (9557): 186–7, author reply 187. doi:10.1016/S0140-6736(07)60099-3. PMID 17240276. S2CID 1150239.
- ^ Chown B.; Lewis Grand.; Kaita K. (October 1957). "A new Kell blood-grouping phenotype". Nature. 180 (4588): 711. Bibcode:1957Natur.180..711C. doi:10.1038/180711a0. PMID 13477267.
- ^ Miller LH, Mason SJ, Clyde DF, McGinniss MH (Baronial 1976). "The resistance factor to Plasmodium vivax in blacks. The Duffy-blood-group genotype, FyFy". The New England Journal of Medicine. 295 (6): 302–four. doi:10.1056/NEJM197608052950602. PMID 778616.
- ^ Kwiatkowski DP (August 2005). "How Malaria Has Affected the Human Genome and What Human being Genetics Can Teach Us about Malaria". American Journal of Human Genetics. 77 (2): 171–92. doi:10.1086/432519. PMC1224522. PMID 16001361.
The unlike geographic distributions of α thalassemia, G6PD deficiency, ovalocytosis, and the Duffy-negative blood group are further examples of the general principle that different populations have evolved dissimilar genetic variants to protect against malaria
- ^ "Position statement: Red blood prison cell transfusion in newborn infants". Canadian Pediatric Lodge. April 14, 2014. Archived from the original on 19 May 2018.
- ^ a b Schmidt, P; Okroi, M (2001), "Also sprach Landsteiner – Blood Group 'O' or Blood Group 'Nil'", Infus Ther Transfus Med, 28 (iv): 206–8, doi:10.1159/000050239, S2CID 57677644
- ^ "Your blood – a textbook about blood and claret donation" (PDF). p. 63. Archived from the original (PDF) on June 26, 2008. Retrieved 2008-07-xv .
- ^ Talaro, Kathleen P. (2005). Foundations in microbiology (5th ed.). New York: McGraw-Loma. pp. 510–1. ISBN0-07-111203-0.
- ^ Moise KJ (July 2008). "Management of rhesus alloimmunization in pregnancy". Obstetrics and Gynecology. 112 (1): 164–76. doi:ten.1097/AOG.0b013e31817d453c. PMID 18591322. S2CID 1997656.
- ^ "Rh血型的由來". Hospital.kingnet.com.tw. Archived from the original on 2009-12-11. Retrieved 2010-08-01 .
- ^ Goodell, Pamela P.; Uhl, Lynne; Mohammed, Monique; Powers, Amy A. (2010). "Risk of Hemolytic Transfusion Reactions Post-obit Emergency-Release RBC Transfusion". American Journal of Clinical Pathology. 134 (2): 202–206. doi:ten.1309/AJCP9OFJN7FLTXDB. ISSN 0002-9173. PMID 20660321.
- ^ Mais, Daniel (2014). Quick compendium of clinical pathology. United States: American Society for Clinical Pathology Printing. ISBN978-0-89189-615-9. OCLC 895712380.
- ^ Possible Risks of Blood Production Transfusions Archived 2009-xi-05 at the Wayback Machine from American Cancer Society. Last Medical Review: 03/08/2008. Last Revised: 01/13/2009
- ^ seven adverse reactions to transfusion Archived 2015-11-07 at the Wayback Machine Pathology Department at University of Michigan. Version July 2004, Revised 11/v/08
- ^ Nickel RG; Willadsen SA; Freidhoff LR; et al. (August 1999). "Conclusion of Duffy genotypes in 3 populations of African descent using PCR and sequence-specific oligonucleotides". Human Immunology. threescore (8): 738–42. doi:ten.1016/S0198-8859(99)00039-7. PMID 10439320.
- ^ Bruce, MG (May 2002). "BCF – Members – Chairman'southward Annual Report". The Claret Care Foundation. Archived from the original on April 10, 2008. Retrieved 2008-07-fifteen .
As Rhesus Negative blood is rare among local nationals, this Agreement volition be of item value to Rhesus Negative expatriates and travellers
- ^ Freeborn, Donna. "Hemolytic Disease of the Newborn (HDN)". University of Rochester Medical Center. Archived from the original on 19 September 2016. Retrieved 30 November 2020.
- ^ a b East.A. Letsky; I. Leck; J.1000. Bowman (2000). "Chapter 12: Rhesus and other haemolytic diseases". Antenatal & neonatal screening (2nd ed.). Oxford Academy Press. ISBN978-0-19-262826-8.
- ^ Daniels G, Finning K, Martin P, Summers J (September 2006). "Fetal claret grouping genotyping: present and future". Annals of the New York Academy of Sciences. 1075 (ane): 88–95. Bibcode:2006NYASA1075...88D. doi:10.1196/annals.1368.011. PMID 17108196. S2CID 23230655.
- ^ "Utilize of Anti-D Immunoglobulin for Rh Prophylaxis". Royal College of Obstetricians and Gynaecologists. May 2002. Archived from the original on December 30, 2008.
- ^ "Pregnancy – routine anti-D prophylaxis for D-negative women". NICE. May 2002. Archived from the original on 2022-02-05. Retrieved 2022-02-11 .
- ^ a b American Clan of Blood Banks (24 Apr 2014), "V Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Association of Blood Banks, archived from the original on 24 September 2014, retrieved 25 July 2014 , which cites
- The Principal Medical Officer's National Claret Transfusion Commission (c. 2008). "The appropriate use of group O RhD negative reddish cells" (PDF). National Health Service. Archived from the original (PDF) on 9 August 2014. Retrieved 25 July 2014.
- ^ "RBC compatibility table". American National Red Cross. December 2006. Archived from the original on 2008-09-13. Retrieved 2008-07-fifteen .
- ^ Blood types and compatibility Archived 2010-04-xix at the Wayback Machine bloodbook.com
- ^ "Blood Component ABO Compatibility Chart Ruddy Blood Cells and Plasma". Blood Banking company Labsite. Academy of Michigan. Archived from the original on 16 June 2019. Retrieved sixteen December 2014.
- ^ "Plasma Compatibility". Matching Blood Groups. Australian Red Cross. Archived from the original on seven May 2020. Retrieved xix June 2020.
- ^ Fauci, Anthony S.; Eugene Braunwald; Kurt J. Isselbacher; Jean D. Wilson; Joseph B. Martin; Dennis L. Kasper; Stephen L. Hauser; Dan Fifty. Longo (1998). Harrison'due south Principals of Internal Medicine . McGraw-Hill. p. 719. ISBN0-07-020291-v.
- ^ "Universal acceptor and donor groups". Webmd.com. 2008-06-12. Archived from the original on 2010-07-22. Retrieved 2010-08-01 .
- ^ Anstee DJ (2009). "Red prison cell genotyping and the future of pretransfusion testing". Claret. 114 (2): 248–56. doi:10.1182/blood-2008-11-146860. PMID 19411635. S2CID 6896382.
- ^ Avent ND (2009). "Big-scale blood grouping genotyping: clinical implications". Br J Haematol. 144 (1): 3–13. doi:ten.1111/j.1365-2141.2008.07285.x. PMID 19016734.
- ^ Landsteiner K (1900). "Zur Kenntnis der antifermentativen, lytischen und agglutinierenden Wirkungen des Blutserums und der Lymphe". Zentralblatt für Bakteriologie, Parasitenkunde und Infektionskrankheiten. 27: 357–362.
- ^ Kantha, S.S. (1995). "The blood revolution initiated by the famous footnote of Karl Landsteiner's 1900 paper" (PDF). The Ceylon Medical Journal. 40 (3): 123–125. PMID 8536328. Archived (PDF) from the original on 2018-08-30. Retrieved 2018-06-01 .
- ^ Landsteiner, Karl (1961) [1901]. "On Agglutination of Normal Human Claret". Transfusion. ane (ane): 5–8. doi:x.1111/j.1537-2995.1961.tb00005.ten. PMID 13758692. S2CID 40158397Originally published in German in Wiener Klinische Wochenschrift, 46, 1132–1134
{{cite periodical}}: CS1 maint: postscript (link) - ^ Farhud, D.D.; Zarif Yeganeh, G. (2013). "A brief history of human blood groups". Iranian Journal of Public Health. 42 (1): 1–6. PMC3595629. PMID 23514954.
- ^ Von Decastello, A.; Sturli, A. (1902). "Concerning isoagglutinins in serum of salubrious and sick humans". Munchener Medizinische Wochenschrift. 26: 1090–1095.
- ^ a b c Farr AD (April 1979). "Blood group serology—the first four decades (1900–1939)". Medical History. 23 (2): 215–26. doi:10.1017/s0025727300051383. PMC1082436. PMID 381816.
- ^ Janský J. (1907). "Haematologick studie u. psychotiku". Sborn. Klinick (in Czech). 8: 85–139.
- ^ Garratty, G.; Dzik, W.; Issitt, P.D.; Lublin, D.Chiliad.; Reid, Thou.E.; Zelinski, T. (2000). "Terminology for blood grouping antigens and genes-historical origins and guidelines in the new millennium". Transfusion. 40 (4): 477–489. doi:10.1046/j.1537-2995.2000.40040477.x. PMID 10773062. S2CID 23291031. Archived from the original on 2022-02-fifteen. Retrieved 2022-02-eleven .
- ^ Moss W.L. (1910). "Studies on isoagglutinins and isohemolysins". Bulletin of the Johns Hopkins Infirmary. 21: 63–lxx.
- ^ Farr Advertizement (April 1979). "Blood group serology—the starting time four decades (1900–1939)". Medical History. 23 (2): 215–26. doi:10.1017/S0025727300051383. ISSN 0025-7273. PMC1082436. PMID 381816.
- ^ Kennedy, James A. (1929-02-23). "Claret grouping classifications used in hospitals in the United States and Canada: Final Report". Periodical of the American Medical Association. 92 (8): 610. doi:10.1001/jama.1929.02700340010005. Archived from the original on 2022-02-15. Retrieved 2022-02-xv .
- ^ Garratty, G.; Dzik, W.; Issitt, P. D.; Lublin, D. M.; Reid, M. E.; Zelinski, T. (2000). "Terminology for blood grouping antigens and genes-historical origins and guidelines in the new millennium". Transfusion. xl (4): 477–489. doi:ten.1046/j.1537-2995.2000.40040477.ten. PMID 10773062. S2CID 23291031. Archived from the original on 2021-08-30. Retrieved 2021-08-30 .
- ^ Doan, C.A. (1927). "The Transfusion problem". Physiological Reviews. vii (i): ane–84. doi:x.1152/physrev.1927.vii.ane.1. ISSN 0031-9333.
- ^ a b Okroi, Mathias; McCarthy, Leo J. (July 2010). "The original blood group pioneers: the Hirszfelds". Transfusion Medicine Reviews. 24 (3): 244–246. doi:10.1016/j.tmrv.2010.03.006. ISSN 1532-9496. PMID 20656191. Archived from the original on 2021-08-thirty. Retrieved 2021-08-thirty .
- ^ Schmidt, P.; Okroi, M. (2001). "Besides sprach Landsteiner – Claret Group 'O' or Blood Group 'NULL'". Transfusion Medicine and Hemotherapy. 28 (4): 206–208. doi:10.1159/000050239. ISSN 1660-3796. S2CID 57677644.
- ^ Goodman, Neville M. (1940). "Nomenclature of Claret Groups". British Medical Periodical. 1 (4123): 73. doi:10.1136/bmj.1.4123.73-a. PMC2176232.
- ^ Garratty, G.; Dzik, Westward.; Issitt, P.D.; Lublin, D.Chiliad.; Reid, M.E.; Zelinski, T. (2000). "Terminology for claret group antigens and genes-historical origins and guidelines in the new millennium". Transfusion. 40 (4): 477–489. doi:ten.1046/j.1537-2995.2000.40040477.x. ISSN 0041-1132. PMID 10773062. S2CID 23291031.
- ^ Dungern, Due east.; Hirschfeld, L. (1911). "Über Vererbung gruppenspezifischer Strukturen des Blutes". Zeitschrift für Induktive Abstammungs- und Vererbungslehre (in High german). v (1): 196–197. doi:10.1007/BF01798027. S2CID 3184525. Archived from the original on 2022-02-15. Retrieved 2022-02-11 .
- ^ Landsteiner, K.; Levine, P. (1927). "A New Agglutinable Factor Differentiating Individual Man Bloods". Experimental Biology and Medicine. 24 (six): 600–602. doi:10.3181/00379727-24-3483. S2CID 87597493.
- ^ Landsteiner, M.; Levine, P. (1927). "Further Observations on Individual Differences of Human Blood". Experimental Biology and Medicine. 24 (ix): 941–942. doi:x.3181/00379727-24-3649. S2CID 88119106.
- ^ Coombs RR, Mourant AE, Race RR (1945). "A new test for the detection of weak and incomplete Rh agglutinins". Br J Exp Pathol. 26: 255–66. PMC2065689. PMID 21006651.
- ^ a b "Despite scientific debunking, in Japan yous are what your blood blazon is". MediResource Inc. Associated Printing. 2009-02-01. Archived from the original on September 28, 2011. Retrieved 2011-08-xiii .
- ^ Nuwer, Rachel. "Y'all are what y'all bleed: In Nihon and other east Asian countries some believe blood type dictates personality". Scientific American. Archived from the original on 10 January 2012. Retrieved sixteen Feb 2011.
Further reading [edit]
- Dean, Laura (2005). Blood Groups and Red Jail cell Antigens, a guide to the differences in our claret types that complicate claret transfusions and pregnancy. Bethesda Dr.: National Center for Biotechnology Data. ISBN1-932811-05-2. NBK2261.
- Mollison PL, Engelfriet CP, Contreras M (1997). Blood Transfusion in Clinical Medicine (10th ed.). Oxford UK: Blackwell Scientific discipline. ISBN0-86542-881-half dozen.
External links [edit]
- BGMUT Blood Group Antigen Gene Mutation Database at NCBI, NIH has details of genes and proteins, and variations thereof, that are responsible for claret types
- Online Mendelian Inheritance in Man (OMIM): ABO Glycosyltransferase; ABO - 110300
- Online Mendelian Inheritance in Human (OMIM): Rhesus Blood Grouping, D Antigen; RHD - 111680
- "Blood group test". Gentest.ch GmbH. Archived from the original on 2017-03-24. Retrieved 2017-03-23 .
- "Blood Facts – Rare Traits". LifeShare Blood Centers. Archived from the original on September 26, 2006. Retrieved September fifteen, 2006.
- "Modern Human Variation: Distribution of Claret Types". Dr. Dennis O'Neil, Behavioral Sciences Section, Palomar Higher, San Marcos, California. 2001-06-06. Archived from the original on 2001-06-06. Retrieved November 23, 2006.
- "Racial and Ethnic Distribution of ABO Blood Types – BloodBook.com, Blood Information for Life". bloodbook.com. Archived from the original on 2010-03-04. Retrieved September 15, 2006.
- "Molecular Genetic Ground of ABO". Retrieved July 31, 2008.
Source: https://en.wikipedia.org/wiki/Blood_type
0 Response to "Can Two a Positiveblood Types Have a a Negative Baby"
Post a Comment